Menu
SLOWING THE AGING PROCESS WITH NATURAL PROGESTERONE
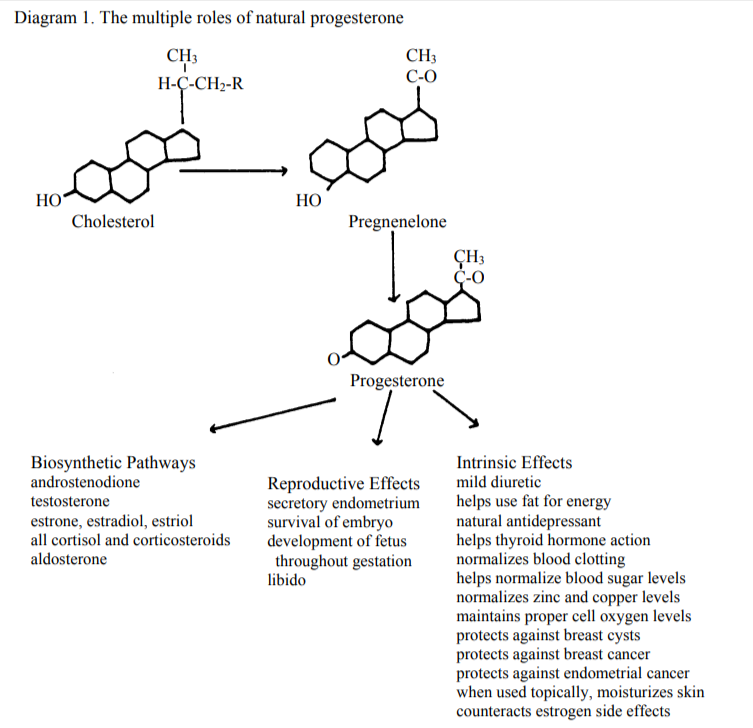
Overview of Progesterone
Aging is as inevitable as death and taxes, but prevention of premature aging is a goal to
which we all should (and can) aspire. In this regard, the role of natural progesterone should
be re-examined. In women, progesterone and estrogen are produced primarily by the ovary
during normal menstrual cycles. Progesterone maintains the secretory endometrium and, in
the case of a fertilized ovum, is necessary for the survival of the embryo and the development
of the growing fetus throughout gestation. Also, progesterone is an important precursor in
the biosynthesis of adrenal corticosteroids and of all the sex hormones, and provides many
important intrinsic physiological functions, the lack of which can lead to symptoms often
associated with aging as well.
Thus, natural progesterone is one of the body’s most important hormones and has benefits
far beyond its role in menstrual cycles and pregnancy. As menopause approaches and the
number of ovarian follicles decrease, progesterone levels also decrease. With menopause,
progesterone levels fall close to zero, whereas some estrogen continues to be synthesized
within fat and muscle cells. The pre and postmenopausal loss of progesterone can be
correlated not only with osteoporosis, but with many bodily changes commonly interpreted
as aging. Proper supplementation with natural progesterone prevents and commonly reverses
these supposed aging effects. Good health during the latter half of one’s life is not a forlorn
hope; it can become a reality if we learn to support rather than impair or neglect our natural
health giving capabilities. In this regard, natural progesterone has a key role.
[Natural progesterone should not be confused with the synthetic progesterone promoted by
the pharmaceutical industry and so often prescribed by physicians as progesterone
substitutes. The truth is that these synthetic versions do not duplicate natural progesterone’s
full spectrum of benefits, and all carry multiple potential undesirable side effects. This will
be more fully discussed later in the paper.]

Comparing Estrogen and Progesterone
Our present preoccupation with supplemental estrogen and our neglect of natural
progesterone is a medical oddity peculiar to the past 3-4 decades. The reasons for this are
complex, but include incomplete knowledge among most physicians and the pressures on
research funds driven by pharmaceutical profits. At this time, it is important to understand
the known physiological effects of these two important hormones
Comparing Estrogen and Progesterone
Estrogen effects
- breast stimulation
- creates proliferative endometrium
- salt and fluid retention
- increased fat in body
- depression and headaches
- interferes with thyroid hormone
- increased blood clotting
- decreases libido
- impairs blood sugar control
- loss of zinc and retention of copper
- reduced oxygen levels in all cells
- causes endometrial cancer
- increased risk of breast cancer
- slightly restrains osteoclast function
Progesterone effects
- protects against breast fibrocysts
- maintains secretory endometrium
- natural diuretic
- helps use fat for energy
- natural anti-depressant
- facilitates thyroid hormone utilization
- normalizes blood clotting
- restores libido
- normalizes blood sugar levels
- normalizes zinc and copper levels
- restores proper cell oxygen levels
- prevents endometrial cancer
- helps prevent breast cancer
- stimulates osteoblast bone building
- necessary for survival of embryo
- precursor of cortisone and sex hormones
Further, estrogen is an end-product hormone and does not participate in the biosynthesis of
other hormones or active compounds; whereas progesterone, while active in its own right,
also is a precursor to other vital hormones in the body
When one observes the many benefits of progesterone, one must wonder why this valuable
hormone has been so long neglected. Let us more closely review the various roles of natural
progesterone
Progesterone in the Menstrual Cycle
The female role in the propagation of the human species includes, of course, the menstrual
cycle. Both sets of ovarian hormones, estrogens and progesterone, are pare of a complex,
interconnected and closely coordinated system of hypothalamic brain centers and pituitary
hormones involving feedback controls designed to produce a wide array of physiological
effects, the purpose of which is to prepare the uterus (and the body as well) for pregnancy
and to produce an ovum ready for fertilization by sperm. Simply put, hypothalamic nuclei
within the limbic brain monitor serum levels of estrogen and progesterone; when levels fall
(bringing on menstruation), the hypothalamic nuclei produces gonadotropin releasing
hormone (GnRH) which causes the pituitary secretion of follicle stimulating hormone
(FSH) which stimulates the ovary to synthesize estrogen which (a) initiates proliferation
of the endometrium, and (b) initiates ovarian follicles to prepare an ovum for ovulation. As
the follicle matures in this activity, pituitary luteinizing hormone (LH) rises to a peak
coinciding with ovulation. With ovulation, the successful ovarian follicle becomes the
corpus luteum which then synthesizes progesterone, often as much as 20-25 mg per day.
Progesterone transforms the proliferative endometrium into the secretory form necessary for
successful implantation of a fertilized ovum, should one occur. If fertilization does not occur
in a week or so, the levels of both ovarian hormones decline, leading to menstruation, and the
cycle begins anew.
In this system, estrogen is the dominant hormone during the first two weeks of the cycle
(prior to ovulation) and, after ovulation, progesterone soon becomes the dominant hormone.
If fertilization does not occur, progesterone declines after day 26 or 27 of the typical
menstrual cycle, bringing on menstruation.
In the event of a successful fertilization of an ovum and its implantation in the uterus,
progesterone secretion by the corpus lelteum is enhanced by a hormone (chorionic
gondotropin) produced by the developing zygote (fertilized ovum). As the placenta
develops, it takes over production of progesterone, increasing the production greatly. During
the third trimester of pregnancy, for example, placental progesterone production reaches 300-
400 mg per day
Interestingly, all the ovarian follicles from which future ova will spring are present in the
ovaries at birth. In fact, there may be 300,000 follicles initially present. With the onset of
puberty (menarche) and the monthly surges of follicle stimulating hormone (FSH) and
luteinizing hormone (LH), the monthly development of ova begins. One would think that the
plentiful initial supply of follicles would yield ova sufficient to last until the cessation of
menstrual cycles (menopause) at age 50-55. This, however, is not the case in North America.
It has become quite common that unusual follicle “burn-out” occurs as early as age 35 and
thus many women have anovulatory (and thus, lacking progesterone) cycles for 15 years or
more before actual menopause. This results in sustained monthly estrogen dominance,
leading to a wide variety of medical problems stemming from unopposed estrogen side
effects. Such women present with water retention, increased fat deposition about the hips
and lower abdomen, hypertension, lack of libido, irritability and depression, fibrocystic
breasts, endometrial cancer and breast cancer
Since these complaints are far less common in “undeveloped” countries, it is natural to
speculate that the cause of follicle burn-out is environmental, probably a toxic contaminant to
which we are exposed, or possibly some dietary deficiency. The leading candidates for this
endemic malady at this time are our pervasive petrochemical derivatives, principally the
petrochemically derived insecticides and herbicides which, being fat-soluble, become
concentrated in animal fat food chain products. Many of these compounds act as estrogen
mimics and, in this regard are amazingly potent, being active at nanogram (one-billionth
[109
] of a gram) levels. They include pesticides such as DDT, DDE, Kepone, dieldrin,
dicofol, and methoxychlor; and polychlorinated biphenyls (PCB’s), anthracene, alkyl phenols
and bisphenol A (the monomer that is condensed to make polycarbonate plastic). These estrogen mimics are highly lipophilic (fat soluble), very persistent (not biodegradable or well
excreted), and accumulate in fat tissue of animals and humans over a lifetime. 1,2
The toxicity of DDT was recognized sometime ago and its use has been severely restricted
in the US and European countries. However, it is still being used in third world countries,
especially for mosquito control, and new DDT production plants are still being funded by the
World Bank. The DDT does not remain in the country where it is used. It, or its metabolite,
DDE, can be carried by the wind to incorporation in the food chain of all sea life, including
the fish we eat; and its use on food crops becomes international when the foods are sold
worldwide. The other pesticides, PCB’s, and plastics are particularly prevalent in our society
today and the full panoply of their toxic results is yet to be revealed.
Thus, it should be clear that anovulatory cycles, whether created by environmental toxins
or other causes, lead to progesterone deficiency and estrogen dominance, with all its potential
for undesirable side effects. When this hormone imbalance is present, supplementation with
natural progesterone is paramount
Progesterone and Menopause
Menopause, were it only the cessation of menses and the loss of fecundity, would be
viewed with relief by most women. In the US and most “advanced” nations, however,
menopause is viewed as a portent of disagreeable symptoms and progressive physical
deterioration. The prospect of unpredictable hot flushes, night sweats and mood swings, and
the seemingly inevitable progress of osteoporosis with its ultimate consequence of fracture is
troublesome, if not downright fearsome. Estrogen supplementation may reduce hot flushes
and can, for a while, slow osteoporotic bone loss. However, estrogen also increases one’s
risk of fibrocystic breast, edema, uterine fibroids, endometrial cancer, and most probably,
breast cancer. Menopause is a continental divide in a woman’s life beyond which the view is
one of trouble and eventual disaster. In large pare, this bleak outlook is due, in reality, to our
present neglect of using natural progesterone.
Menopause results from lowered estrogen levels such that monthly blood-rich
endometrial development and its shedding does not occur. It does not mean that estrogen
levels have fallen to zero. Estrogen continues to be produced, in somewhat lesser amounts,
by conversion of a sterol, androstenedione, which is found in fat, including the fat in our
muscle cells. Menopause merely means that ovarian production of estrogen declines to
levels which do not induce endometrial response. It is a natural phenomenon indicating only
that one’s period of fertility is over.
Of greater importance is the fact that, in the US, it is common that women’s production of
progesterone falls to near zero at least 6-8 years before actual menopause, due to the
anovulatory periods described above. This is rarely recognized by typical physicians who
more or less automatically prescribe estrogen for many “menopausal” symptoms which, in actuality, result from progesterone deficiency, not estrogen deficiency. Not only are women
subject to estrogen dominance and its attendant symptoms, but they arrive at menopause with
osteoporosis well underway, a clear indication that osteoporosis is not due to estrogen
deficiency, but more likely due to progesterone deficiency (see below). All this could be
prevented by timely supplementation during the menstrual cycle of natural progesterone
during the pre and peri-menopausal period.
Progesterone and Osteoporosis
The doctor is told that estrogen helps delay osteoporosis, is good for hot flashes, and may
help prevent cardiovascular disease; and that these benefits outweigh the various estrogen
risks suck as fibroids, breast fibrocysts and/or cancer, and endometrial cancer. He is further
told that synthetic progesterone will decrease estrogen’s risk of endometrial cancer and that it
is up to the patient to decide if she is willing to accept the risks of progestin’s side effects.
The fact is, there is a degree of falsity in each of these claims. For now, let us focus on the
osteoporosis problem.
Bones are living tissue, constantly being made, unmade (resorbed), and made anew. They
can be broken and then healed; they can grow as we grow; and they can restore their minerals
when such are taken from them. Within bones are cells (osteoblasts) that make new bone;
and there are cells (osteoclasts) that resorb bone previously made. Bone mass and bone
mineral density represent the relative contribution of osteoclast-mediated bone resorption and
osteoclast-mediated new bone formation. Others factors remaining equal, bones remain
stable when osteoblast and osteoclast actions are in equilibrium. Osteoporosis is a condition
involving relative osteoblast deficiency.
The only proven bone function of estrogen is to deter osteoclast-mediated bone
resorption.3
Progesterone, on the other hand, stimulates osteoblast-mediated new bone
formation.4
At menopause, the decline of estrogen levels allow a temporary increase in bone
resorption; estrogen supplementation will retard this accelerated bone loss but it will not
stimulate new bone formation and thus can not correct the loss that has occurred. Five years
after menopause, this benefit of estrogen disappears; with or without estrogen supplements,
bone loss progresses at the same rate (of approximately 1.5% per year). 5
Bone formation in the adult woman is the function of progesterone, not estrogen. In my
clinical experience since 1982, I have found that osteoporosis can be reversed in many
women by restoring adequate natural progesterone, along with a program of diet, a few
vitamin and mineral supplements and exercise. Several of the synthetic progestins have a
modest effect6,7 (at most a 5% increase bone mass in two years), but none are as effective as
natural progesterone is (typically a 15% increase in 2-3 years), depending on degree of
previous bone loss) with or without supplemental estrogen8,9. Further, the progestins are
known to cause many side effects, whereas natural progesterone has no known side effects.
Progesterone and Hot Flushes
Hot flushes (or flashes) are vasomotor disturbances emanating from homeostatic control
centers within the hypothalamus leading to inappropriate dilation of skin capillaries and/or
sweating. During menopause, they correlate with high levels of pituitary follicle stimulating
hormone (FSH), resulting from low estrogen and progesterone levels. When estrogen is
supplemented, FSH levels fall and so does the incidence of hot flushes. The most likely
scenario for this phenomenon is that low hormone levels stimulate the hypothalamic centers
resulting not only the FSH elevation, but also the activation of nearby hypothalamic neural
nuclei controlling vasomotor responses. Although estrogen supplementation is effective in
reducing hot flushes, later attempts to reduce estrogen supplementation often results in
recurrence of the symptoms.
There are other ways to deal with hot flushes. Experience shows that a diet rich in fresh
vegetables and low in sugar and refined carbohydrates, along with vitamin E and aerobic
exercise, will often decrease the intensity and frequency of these symptoms. Also,
replacement of natural progesterone alone and in sufficient doses will frequently result in
elimination or decreased severity of hot flushes. Since the hypothalamic centers monitor
both estrogen and progesterone, it should not be surprising that sufficient natural
progesterone will be effective in treating hot flushes. Because of the inherent toxicity of
unopposed estrogen, these methods should be thoroughly tried before resorting to estrogen
supplements.
Cardiovascular Risks of Estrogen
Recent pharmaceutical advertisements claim that estrogen supplementation reduces the
risk of cardiac death. Despite the evidence of numerous studies showing otherwise,10-13 this
claim is based on a nurses questionnaire report which found a slightly lower incidence of
cardiac deaths in estrogen using nurses, compared to non-estrogen using nurses. In this
report,14 the total number of cardiac deaths among the nurse population constitutes less than
0.5% of the total number in the study. Further, it is revealed that among the nurses for whom
estrogen had not been prescribed, there was a higher proportion of nurses with diabetes,
obesity, cigarette smoking and little or no exercise. These are all risk factors for heart
disease, and therefore the doctors for these nurses had wisely refrained from prescribing
estrogen for them. The claim of lower relative risk for estrogen users is based solely on the
statistical “adjustment” of the risk factors listed above. With a slightly different
“adjustment”, the putative estrogen benefit disappears.
Furthermore, the pharmaceutical advertisements do not mention the fact the ischemic
(thrombo-embolic) stroke death incidence was higher among the estrogen users. This is
entirely understandable since estrogen increases the tendency of blood to form clots. If one
is offered estrogen supplements, shouldn’t he/she be told that such treatment increased the
chance of dying from a stroke? Natural progesterone, on the other hand, normalizes blood clotting. The message to be learned is that, if estrogen is to be prescribed, it should always
be accompanied by natural progesterone.

Ovarian Hormones and Fibroids
Fibroids are non-malignant nodules or masses of connective tissue within or extending
from the walls of the uterus. They tend to develop during the pre or peri-menopausal phase
when estrogen is dominant; they atrophy after menopause when estrogen levels fall. Proper
supplementation with natural progesterone during these critical times of estrogen dominance
will prevent or reduce the size of uterine fibroids. If a woman can prevent or reverse
osteoporosis by using natural progesterone instead of estrogen replacement therapy (ERT),
she need not risk the development of fibroids.
Progesterone Prevention of Fibrocystic Breasts and Mastodynia
Estrone and estradiol, the two estrogens most often prescribed in ERT, both stimulate
breast tissue, especially if unopposed by natural progesterone. Thus, during the
premenopausal estrogen-dominant phase, breast fibrocysts and painful breast swelling
(mastodynia) are common. These problems are perpetuated after menopause by ERT. The
presence of fibrocystic breasts in the premenopausal phase is sufficient evidence of
unopposed estrogen and should be treated with adequate natural progesterone
supplementation. When this is done, the fibrocystic problem usually disappears in 2-3
months, as does mastodynia. Very few medical conditions are this easy to treat. It is
staggering to consider the many women who suffer needlessly from these problems.
Ovarian Hormones and Breast Cancer
The cause of causes of breast cancer are not known. Some argue that dietary fats (such as
the trans-fatty acids) are involved, but the available references are mixed. More recently, a
correlation between certain environmental pesticides (especially the fat-soluble ones) and
other petrochemical derivatives with breast cancer incidence has begun to attract attention.
Many of these chemicals act as extremely potent estrogen mimics, are lipophilic, and
accumulate in fat tissue in animals and humans. The importance of these chemicals in
explaining the rising incidence of breast cancer may be appreciated by understanding the
worrisome connection between estrogen and breast cancer. Consider the following evidence:
- Early pregnancy conveys protection against breast cancer; women bearing their first child after age 30 have a higher risk than nulliparous women.
- Only the first, full term, early pregnancy conveys protection; aborted or interrupted pregnancies do not afford protection.
- Married women without children are at a higher risk than those with one or more children; unmarried women and nuns are a higher risk than women who have experienced pregnancy.
- The risk of breast cancer is significantly less in women subjected to oophorectomy prior to their fortieth year.
- Protective effect of early oophorectomy are negated by supplemental estrogen (ERT).
- Treatment of males with estrogen (for prostate cancer or after trans-sexual surgery) is associated with an increased risk of breast cancer.
- Survival time after mastectomy for cancer is improved by Tamoxifen, a weak estrogen that acts as an anti-estrogen to inhibit estrogen receptors.
Ovarian Hormones and Endometrial Cancer
The only known cause of endometrial cancer is unopposed estrogen. Since the mid1970’s, it has been known that estrogen should never be given without being opposed by
supplemental progesterone or one of the progestins. The work of Gambrell,17 for example, is
especially important in illustrating this cancer risk of unopposed estrogen and the protection
by progestin supplementation. Further, Hargrove18 showed the superiority of natural
progesterone over progestins by comparing the endometrial effects of (a) progestin
[medroxyprogesterone acetate] given with estrone, to that of (b) natural progesterone when
given with estradiol. He found that estradiol and natural progesterone supplementation in
menopausal women resulted in symptomatic improvement, minimal side effects, an improved
lipid profile, and amenorrhea without endometrial proliferation or hyperplasia (emphasis
added). Endometrial proliferation and/or hyperplasia are considered to be early steps in the
endometrial cellular changes that can lead to cancer.
From what is already known, one could reasonably hope that if clinicians were alert to the
estrogen dominance that can occur in premenopausal women and would supplement them
with natural progesterone, the risk of endometrial cancer would be dramatically reduced,
perhaps to zero.
Health Risks of Progestins
Progestin (also called progestagen or gestagen) refers to the class of synthetically created
patentable compounds which share the ability to sustain human secretory endometrium and,
if given early enough in the menstrual cycle, to prevent ovulation. In this they are similar to
natural progesterone, the specific hormone produced by the corpus luteum after ovulation and
also by the placenta. Progestins are widely used in oral contraceptives and in hormone
replacement therapy (HRT). In medical and lay writing, many authors confuse the two
words, progestin and progesterone. This is a great error, since they are not the same and
differ in many important aspects. Progestins are foreign to all living things and have atoms
introduced at unusual positions in their molecules such that their metabolism and excretion
are inhibited and they induce actions not consistent with natural progesterone. Specifically,
they lack intrinsic physiologic benefits of progesterone, they can not function in the major
biosynthetic pathways as progesterone does, and they carry a wide array of potential
undesirable side effects.
One of the most commonly used progestins, medroxyprogesterone acetate (Provera),
carries the warning that its use in women during early pregnancy can increase the risk of
early abortion or cause congenital abnormalities in the fetus. Since natural progesterone is
necessary for the survival of the embryo and the normal development of the fetus throughout
pregnancy, it is clear that Provera is not progesterone. A partial list of progestin side effects
follows:
POTENTIAL SIDE EFFECTS OF SYNTHETIC PROGESTINS
Warnings:
- Increased risk of birth defects such as heart and limb defects if taken during the first four months of pregnancy.
- Beagle dogs given this drug developed malignant mammary nodules.
- Discontinue this drug if there is sudden or partial loss of vision.
- This drug passes into breast milk, consequences unknown.
- May contribute to thrombophlebitis, pulmonary embolism, and cerebral thrombosis.
Contraindications:
Thrombophlebitis, thromboembolic disorders, cerebral apoplexy, liver dysfunction or
disease, known or suspected malignancy of breast or genital organs, undiagnosed vaginal bleeding,
missed abortion or known sensitivity.
Precautions:
- May cause fluid retention, epilepsy, migraine, asthma, cardiac or renal dysfunction.
- May cause breakthrough bleeding or menstrual irregularities.
- May cause or contribute to depression.
- The effect of prolonged use of this drug on pituitary, ovarian, adrenal, hepatic or uterine function is unknown.
- May decrease glucose tolerance, diabetes patients must be carefully monitored.
- May increase the thrombotic disorders associated with estrogens.
Adverse Reactions:
- May cause breast tenderness and galactorrhea.
- May cause sensitivity reactions such as urticaria, pruritis, edema or rash.
- May cause acne, alopecia and hirsutism.
- Edema, weight changes (increase or decrease).
- Cervical erosions and changes in cervical secretions.
- Cholestatic jaundice.
- Mental depression, pyrexia, nausea, insomnia or somnolence.
- Anaphylactic reactions and anaphylaxis (severe acute allergic reactions).
- Thrombophlebitis and pulmonary embolism.
- Breakthrough bleeding, spotting, amenorrhea or changes in the menses.
When taken with estrogen, the following have been observed:
- Rise in blood pressure, headache, dizziness, nervousness, fatigue.
- Changes in libido, hirsutism and loss of scalp hair, decrease in T-3 uptake values.
- Premenstrual-like syndrome, changes in appetite.
- Cystitis-like syndrome.
- Erythema multiforme, erythema nodosum, hemorrhagic eruption, itching.
The reader can note the number of symptoms and medical problems in the list above which
are commonly attributed to aging. Natural progesterone, on the other hand, has no known
side effects. Need more be said?
PMS and Natural Progesterone
Premenstrual syndrome (PMS) refers to a group of symptoms occurring consistently
during the l0-14 days before menses and clearing 2-3 days after the onset of menses. These
symptoms include depression, irritability, anger and other mood swings, headache, fatigue,
edema and a consequent weight gain, and loss of libido. The timing of these symptoms
corresponds precisely to the time when, under normal circumstances, progesterone should be
the dominant hormone. If progesterone is absent, however, then estrogen dominance prevails
throughout the menstrual month. Side effects of unopposed estrogen include many of the
symptoms listed above. In addition, the lack of progesterone would upset the complex
interplay between the hypothalamus and the pituitary, and lead to the full display of PMS symptoms. Thus, PMS may result in whole or in great part from anovulatory cycles in
sensitive women whose emotional and physiological balance is upset by stress and/or
improper diet. When sufficient natural progesterone is supplemented during the 10-14 days
before menses, along with a diet avoiding stimulants, caffeine and sugar, or highly refined
starches, PMS symptoms will disappear or be greatly reduced. In some cases, small
supplements of magnesium and vitamin B6 (pyridoxine) are also helpful.
It should be recalled that the word “syndrome” implies that the etiology and mechanism(s)
of action underlying the disorder are not completely understood or validated by present
scientific research. This should not deter a trial of treatment with natural progesterone. If a
patient’s typical pre-menstrual weight gain is found not to occur when on natural
progesterone treatment, it is objective evidence that estrogen dominance, due to deficiency of
natural progesterone, is playing a strong role, at least in the etiology of the condition.
Further, serum progesterone levels can be obtained during day 20-23 of the cycle; a low
finding corroborates the progesterone deficiency hypothesis.
Other Anti-Aging Benefits of Natural Progesterone
As women approach menopause, they commonly find themselves losing energy, retaining
fluids, fighting fat, developing wrinkles and facial hairs, prone to headaches and depression
and less interest in sex. They see their doctors, take their diuretics and, occasionally, thyroid
medication and face the future with fading enthusiasm. They seek out cosmeticians for their
wrinkles, visit their beauticians more often for their thinning hair, and take calcium
supplements for their thinning bones. What they are unaware of is the importance of proper
hormonal balance, particularly the lack of this singularly important hormone, natural
progesterone. Consider the following:
1. Progesterone is a primary precursor in the biosynthesis of the adrenal corticosteroids.
Without adequate progesterone, syntheses of the cortisones is impaired and the body
turns to an alternative pathway, via adrenal production of dihydro-epiandrosterone
(DHEA) and androstenedione, produced by fat in the body. These alternative pathways
have androgenic side effects which cause the long facial hairs of elderly postmenopausal
women and thinning of their scalp hair. When natural progesterone is supplemented, it is
quite common to witness the disappearance of facial hair and the return of healthy scalp
hair.
Further, impaired corticosteroid production results in a decrease in one’s ability to handle
stress, e.g., surgery, trauma or emotional. With restoration of adequate progesterone, one’s
ability to deal with stress improves.
2. In many peri or post-menopausal women, symptoms of hypothyroidism occur despite
normal serum levels of thyroid hormone. Estrogen interferes with intracellular utilization
of thyroid hormone. Thus, many women with clinical signs of hypothyroidism such as
fatigue, lack of energy, intolerance to cold, etc., are actually suffering from unrecognized
estrogen dominance and will benefit from supplementation with natural progesterone.
Women who are already placed on thyroid supplements will find that their dose can be
reduced or eliminated when natural progesterone is restored to adequate levels. In this
regard, the test for thyroid stimulating hormone (TSH) is a better guide for thyroid
dosage than are the T-3 or T-4 tests.
Estrogen and most of the synthetic progestins increase intracellular sodium and water
uptake. The effect of this on the aldosterone system is hypertension. Since the true cause
is rarely recognized, this condition is called “essential” hypertension by most clinicians
and is commonly treated with diuretics. Natural progesterone, on the other hand, is a
natural diuretic and prevents the cell’s uptake of sodium and water, thus preventing
hypertension. In treating a hypertensive woman taking estrogen and/or a progestin, the
first step should be to discontinue the hormones; the second step is to switch to a diet of
fresh vegetables, eliminating high sodium processed foods and severely limit red meat
from the diet; and the third step is to provide supplemental natural progesterone. In this
manner, drug treatment for hypertension is commonly unnecessary.
3. Whereas estrogen impairs homeostatic control of glucose levels, natural progesterone
stabilizes them, thus, natural progesterone can be beneficial to both those with diabetes
and those with reactive hypoglycemia. Estrogen should be contraindicated in patients
with diabetes.
4. Loss of libido is common with menopause. To the surprise (and delight) of many
postmenopausal women, progesterone often restores normal libido. Estrogen
supplementation, as is known, usually results in a decrease of libido. It is a false
assumption that the enjoyment of full sexual activity is not in the province of postmenopausal women; it is merely a matter of a correctable hormone balance.
5. Thinning and wrinkled skin is a sign of lack of hydration in the skin. It is common in
peri and post-menopausal women and is a sure sign of hormone depletion. Transdermal
natural progesterone is a skin moisturizer. When used as a skin cream, not only is
progesterone well absorbed, but it restores skin hydration . The skin becomes more
youthful in appearance and most small wrinkles disappear.
6. Recent research has found that recovery from brain injury in male test animals is
enhanced by pre-treatment with progesterone. Further, brain cells are well supplied with
progesterone receptors and the brain content of progesterone, as well as pregnenelone and
DHEA, is normally 20-30 times higher than serum levels. It is suggested, therefore, thatprogesterone serves a role in keeping brain cells healthy and that disorders such as
premature senility (Alzheimer’s disease) may be, at least in part, another example of
disease secondary to progesterone deficiency.
Why Natural Progesterone is so Neglected by Contemporary Medicine
It should not require a PhD in physiology to realize that unopposed estrogen is largely
disadvantageous and progesterone is remarkably beneficial. Yet, this view is not shared (or
understood) by many physicians and medical writers. Why should this be? One answer is,
of course, that many doctors have simply not kept up with advances in medical science. The
more sanguine answer is that doctors have come to rely on pharmaceutical advertising as
their education sources and do not fully realize that they, themselves, are the targets of clever
campaigns inducing them to prescribe what the industry sells. Natural progesterone, though
easily and relatively inexpensively derived from plant sterols, (e.g., diosgenin, present in
yams and many other plants) is not offered by the major pharmaceutical firms since, being a
natural substance it is not patentable, and thus not profitable. Natural progesterone is
routinely used by the pharmaceutical industry for synthesis of progestins. The availability
and superiority of natural progesterone is a secret carefully kept from physicians.
Conclusion:
Premature aging remains a great concern in our present society. It is entirely likely that
many factors play a role: nutritional deficiencies, alcoholism, cigarette smoking,
environmental toxins and others may all be implicated. But present knowledge suggests a
large factor is our misdirected attention to estrogen and our neglect of natural progesterone.
Proper understanding and supplementation with natural progesterone promises to restore a
healthy zestful life, where before the only prospect was one of early aging and progressive
deterioration. It is time for natural progesterone to take its place along with proper nutrition,
exercise and a clean environment in the preservation of good health.
Dr. Lee has recently published Natural Progesterone: the Multiple Roles of a Remarkable
Hormone, BLL Publishing, P.O. Box 2068, Sebastopol, CA 95473, recently reviewed by
Townsend Letter for Doctors, April 1994. The reviewer calls it “the most informative and
lucid explanation of the female hormone cycle” that the reviewer had ever encountered and
that it “contains priceless information for women wrestling with the effects of menopause
and hormone imbalance and for the doctors who treat them.”